

Castine Bernardy, graduate research assistant, Department of Civil and Environmental Engineering, University of New Hampshire
Corresponding author James P. Malley Jr., Ph.D., Professor of Civil and Environmental Enginnering, University of New Hampshire
Worldwide concern over the risk of contracting or spreading COVID-19 has sparked widespread interest in using UV devices for air and surface disinfection. The purpose of this Operator’s Corner is to provide tips to the buyers and users of UV devices to inactivate air and surfaces. That market contains thousands of different products and is estimated to be $1 to $2 billion per year in sales. Unfortunately, it lacks uniform validation protocols, manufacturing specifications or guidelines. Hence, it can be the “Wild West” so “Let the Buyer/User Beware.”
Ultraviolet (UV) means many things
Buyers and users need to familiarize themselves in some fashion with the different types of UV including UV-A (wavelength: 315 to 400 nm), UV-B (wavelength: 280 to 315 nm), UV-C (wavelength: 200 to 280 nm) and Vacuum UV (wavelength: 100 to 200 nm). The wavelength ranges given here are based upon IUPAC Gold Book-2020, and for the discussion of disinfection by these UV devices, UV-C wavelengths should be the focus. A subset of that UV-C, which has received some recent attention, is far UV-C (200 to 225 nm) and this, at times, is vaguely and incorrectly simply called far UV. In general, the lower the wavelength, the more energy in the photons of light wave energy being employed by the device.
When discussing the disinfecting power of sunlight, consider a mixture of approximately 95% UV-A and 5% UV-B. Given enough time (days) these wavelengths surely have many effects, but it is a long timeframe and many other factors come into play, such as desiccation of the organisms on a surface, etc.
There are many benefits to sunlight and fresh air, but sunlight is generally not considered as a practical disinfection option due to long timeframes.
All forms of UV have pros and cons, and careful consideration of which UV wavelengths are being used and for what purpose must be done. Dosing human and animal tissues with any forms of UV energy should not be done by buyers and users of these UV devices. Special cases performed by experienced medical professionals under very tightly controlled conditions for very specific medical problems may be found in internet searches, but “do not do this at home” is the best message for all buyers and users of UV devices.
Human and animal tissues should not come in contact with any forms of UV light unless it is performed by a medical facility under the careful control and monitoring by healthcare professionals. The UV devices sold to the public are not carefully regulated, and some advertisements make claims that are not supported by clinical medical trials and testing.
Time is not the most important factor
Often the information provided by advertisements and many very brief user manuals for UV devices simplify operations to talking about time.
All UV professionals recommend that UV device specifications be discussed in terms of delivered dose, since time is not the most important factor. The effectiveness of any UV device or application depends upon at least four key factors: a) the irradiance or fluence rate of the light source at specific wavelength(s) emitted (some refer to this as intensity or strength of light, but those are vague, non-technical terms), b) the optical geometry of the UV device or how it is to be applied, c) the type of organisms to be targeted, including such things as their action spectra and what amount of percent removal (or log inactivation) is desired and d) contact time. Of these lamp characteristics, optical geometry and organism characteristics are far more important than time.
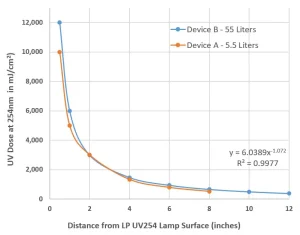
One simple illustration of how lamp geometry matters is distance from the light source, as shown in Figure 1, for two common commercial UV devices (enclosed systems with UV lamps on the top surface of the six-sided treatment area) often sold for medical and laboratory applications. Both contain a common UV lamp (9W, 254 nm low-pressure mercury vapor lamp). Data in Figure 1 is a mathematical model considering UV reflection, refraction absorption air confirmed by UV radiometer readings.
The following case is a practical example as to why time can be a misleading factor. A handheld UV device is developed and tested on a common laboratory bacteria to determine the time needed to inactivate 99.9% of this bacteria (which literature might generically call germs). For the experiment, the UV device is 0.2 inches from the surface coated with the bacteria and it takes 10 seconds to achieve 99.9%, but if the user manual or videos demonstrate that the device should be waved a few inches (three inches) above the surface to be treated for 10 seconds then the reality (Figure 1) would be that the UV dose has dropped off by over 30-fold and now less than 9% of the bacteria are inactivated. The device held six inches away inactivated no bacteria.
Safety concerns
Virtually all UV devices come with warnings about the potential electrical hazards and about the fact that UV light is known to cause harm to skin and eyes. Typical warning labels are shown in Figure 2. Users must be vigilant to protect themselves from all direct, reflected or otherwise stray UV light when using any UV device.
Normal use of UV devices for applying relatively low doses (0 to 100 mJ/cm2) to surfaces or air are being increased 10 to 20-fold (e.g., 2,000 mJ/cm2) to ensure PPE is adequately disinfected before reuse. The elevated doses may result in the unwanted generation of low levels of airborne ozone. Such ozone levels can cause minor irritation to eyes, nose and throat as well as low level headaches if people use these devices for extended periods of time each day.
There may also be impacts of these ozone levels on materials or surfaces being treated, but that has not been verified. The autocatalytic generation and auto-decomposition of ozone created by subjecting air to a typical low-pressure mercury vapor lamp tends to be complicated and affected by many factors.
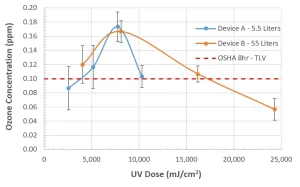
Figure 3 contains the results of an empirical study driven by complaints from users and experimenters working with two typical UV devices being used to disinfect PPE during the COVID-19 pandemic. The data generated is preliminary and reproducible with documented QA/QC but has not been peer reviewed. It is presented here solely as a technical comment of something to be aware of and, if applicable, something to avoid.
Operators Corner focuses on the practical aspects and lessons learned by the owners, operators and providers of UV technology. Authors for these articles are solicited from individuals operating full-scale UV facilities around the globe. Those interested in submitting an applied article, please contact jim.malley@unh.edu.
Contact: cab2020@wildcats.unh.edu; jim.malley@unh.edu