

By Annabelle M. Johnson, Division of Environmental & Ecological Engineering, Purdue University, and corresponding author Ernest R. Blatchley III, Division of Environmental & Ecological Engineering and Lyles School of Civil & Construction Engineering, Purdue University
The global pandemic that started in late 2019 resulted in more than 700 million diagnosed cases of COVID-19 and more than 7 million deaths. 1 The pandemic caused contraction of the global economy, as well as considerable job losses. 2 Through the end of 2023, the cost of COVID-19 to the US economy was estimated to have exceeded $14 trillion. 3 Interestingly, it has been suggested that the cost of pandemic preparedness measures would be roughly 0.2% of the cost of the pandemic itself. 4 Given the scientific consensus that additional pandemics will occur in the future, probably involving airborne respiratory viruses 5, it is prudent to consider measures that can be implemented to combat pandemics, epidemics and other disease outbreaks associated with airborne pathogens.
Currently available engineering interventions that have demonstrated effectiveness for control of airborne pathogens include increased (outdoor) air circulation, filtration and the use of Germicidal Ultraviolet (GUV) devices. Among these, GUV devices have demonstrated the greatest potential for control of airborne pathogens, while also involving lower capital costs and energy consumption than the alternative technologies. 6,7 As such, GUV devices likely are to be key components of systems that are implemented to improve indoor air quality (IAQ) and to control airborne pathogens.
While GUV systems have the potential to play critical roles in the control of airborne pathogens and disease transmission, implementation of these systems has been limited to date. Several factors have contributed to the slow adoption of GUV technologies, including concerns about UV exposure and lack of information to allow for effective decision-making.
To address this issue, a study was conducted to develop quantitative comparisons of the effects of human exposure to UV-C radiation (from properly installed and operated GUV systems) with the effects of more familiar UV exposures. In particular, calculations were conducted to compare the effects of exposure to UV-C radiation, at established exposure limits, with the corresponding damage to exposed tissues associated with exposure to ambient sunlight.
Methodology
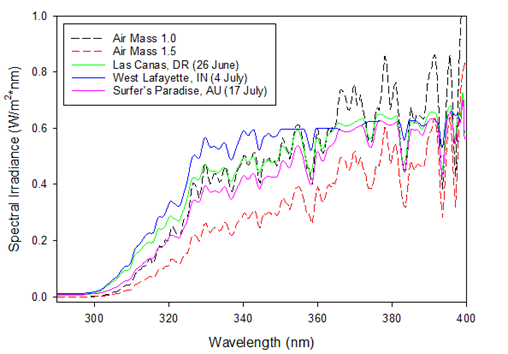
Two different data set types were used to quantify the implications of exposure to ambient solar radiation with respect to different biological responses. The first data set type defined the spectrum of solar radiation received at sea-level altitudes on the earth’s surface. Two solar spectra were used to characterize this exposure: AirMass 1.0 and AirMass 1.5. 8 AirMass 1.0 represents the spectrum of radiation received at sea level on a cloudless day when the sun is directly overhead (i.e., zenith angle = 0°). AirMass 1.5 represents the spectrum of solar radiation received at sea level on a cloudless day for a zenith angle of 48.19°; this spectrum has been identified as a “reasonable average for the 48 contiguous US states over a period of one year.” 8 These reference spectra are made available at wavelengths between 280 nm and 400 nm at an increment of 0.5 nm (see Figure 1).
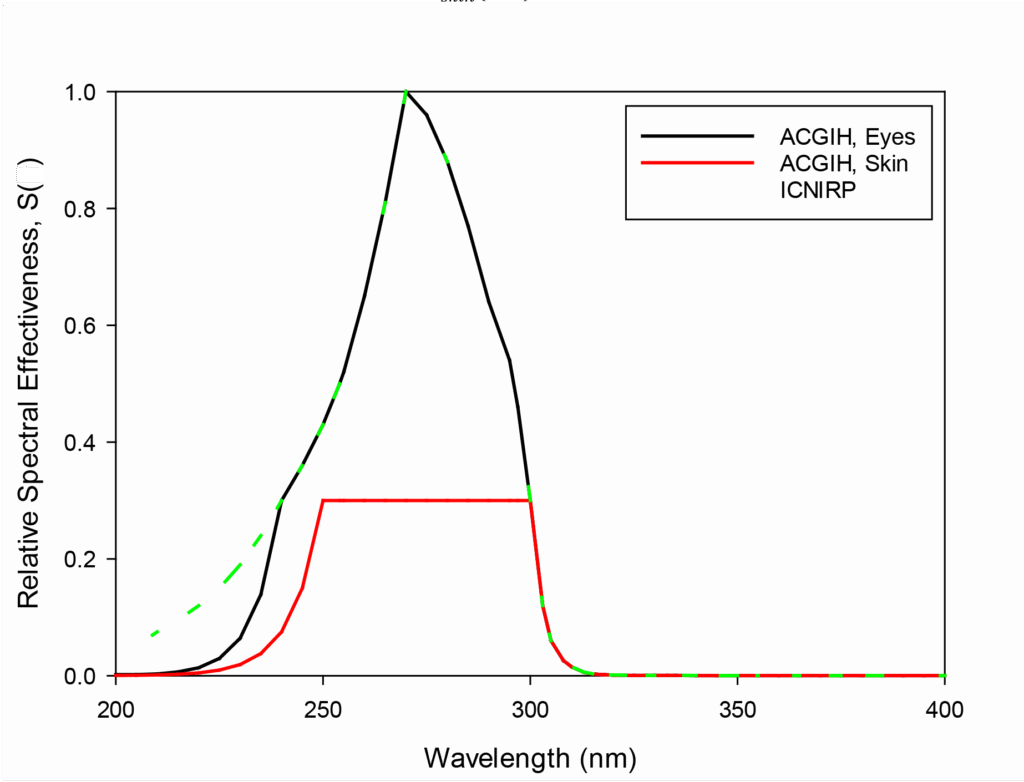
The second data set type illustrates relative spectral effectiveness, which represents the potential for radiation of a given wavelength to produce a given biological response. The American Conference of Governmental Industrial Hygienists (ACGIH) has defined relative spectral effectiveness for damage to skin and eye tissues as a function of wavelength. 9 These spectra are used to define Threshold Limit Values (TLVs) for exposure to UV radiation (see discussion below). Skin and eye relative effectiveness spectra are normalized to 270 nm, where damage to these tissues is maximized; these spectra are illustrated in Figure 2. The data presented in Figure 2 indicate that eye tissues are more sensitive to UV exposure than skin tissue for wavelengths shorter than 300 nm. Above this threshold wavelength, skin and eye susceptibility to UV exposure are indicated to be identical.
The International Commission on Non-Ionizing Radiation Protection (ICNIRP) developed a similar spectrum for human exposure 10; their spectrum is included in Figure 2 for comparison. The ICNIRP spectrum is intended to represent an absolute limit for eye exposure, whereas for skin exposure it defines advisory limits. The ICNIRP definition of relative spectral effectiveness is conservative, relative to the ACGIH spectrum for eyes, for wavelengths less than 240 nm. For wavelengths of 240 nm and longer, the ICNIRP and ACGIH (eye) spectra are identical. All effective dose calculations for skin and eye exposure presented herein are based on the ACGIH definitions of relative spectral effectiveness because they represent the most recently reviewed and revised data regarding the effects of exposure of human tissues to UV radiation.
Radiation at 270 nm is recognized as being efficient at promoting damage to human eye and skin tissues. As such, ACGIH has identified a dose

as an exposure limit for UV-C radiation, based on an assumed exposure period of eight hours; this is identified as a reference dose (DR). The relative spectral effectiveness for eye damage at this wavelength is 1.0 (see Figure 2). The relative spectral effectiveness can be used to calculate the dose at other wavelengths that will yield an equivalent biological response.
To illustrate this calculation, consider the most common source of UV-C radiation used in a GUV application, the low-pressure mercury lamp, which is characterized by essentially monochromatic output at a wavelength of λ = 254 nm. The relative spectral effectiveness for eye damage at this wavelength is 0.5. The TLV for eye exposure at 254 nm (TLV254,eye) can be calculated by dividing the reference dose at λ = 270 nm by the relative spectral effectiveness for eye damage at λ = 254 nm:
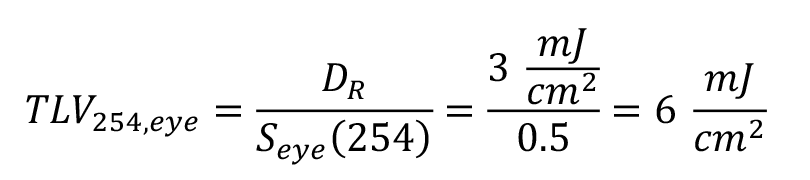
Similarly, the TLV for skin damage at 254 nm (TLV254,skin) can be calculated by dividing the reference dose at λ = 270 nm by the relative spectral effectiveness for skin damage at λ = 254 nm:

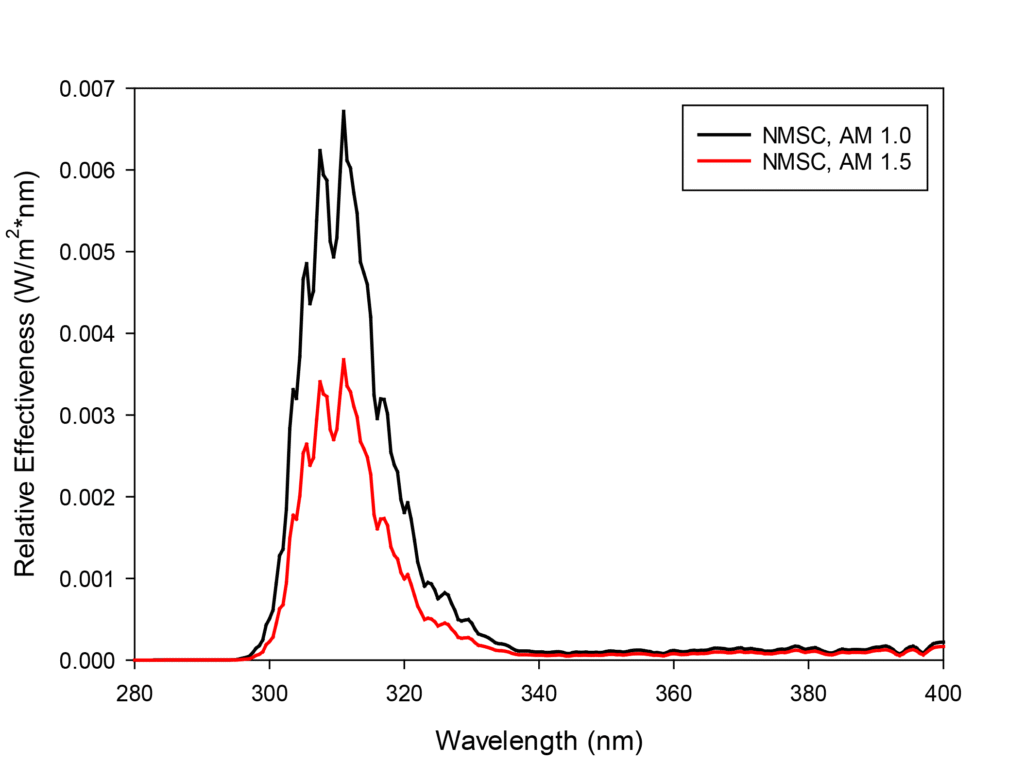
Relative spectral effectiveness also has been defined for non-melanoma skin cancer (NMSC); this spectrum has been normalized to the wavelength corresponding to peak effectiveness (λ = 299 nm). The NMSC relative effectiveness spectrum is illustrated in Figure 3.
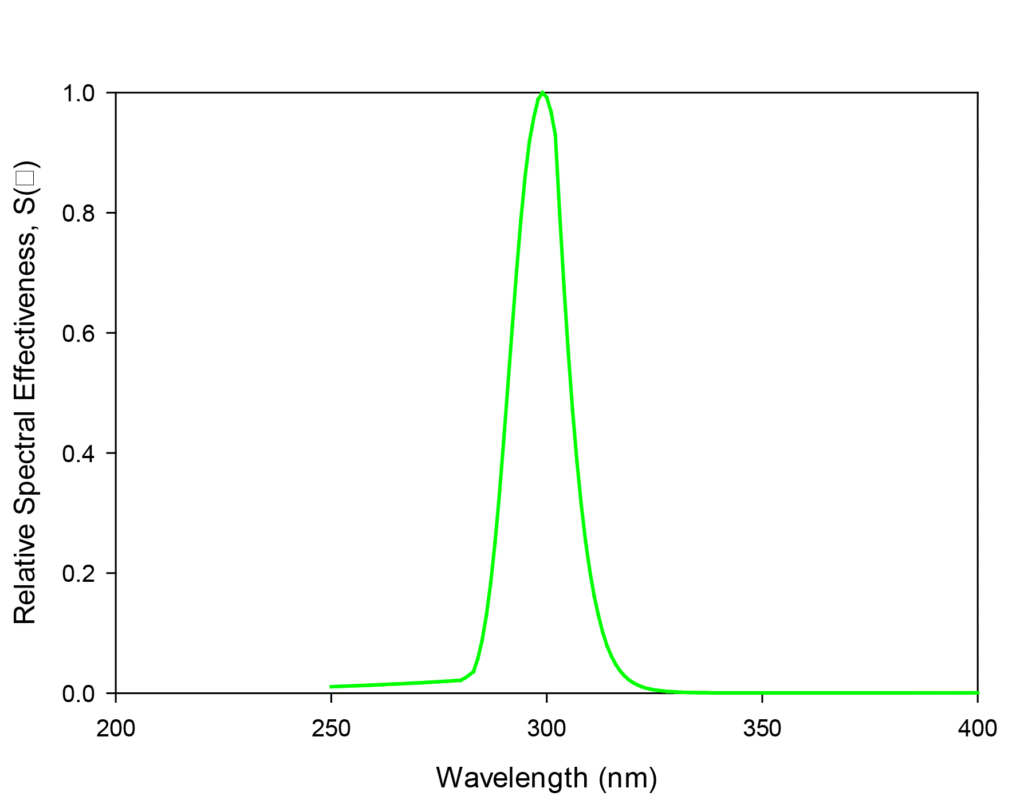
Relative spectral effectiveness for NMSC was developed for radiation in the wavelength range 250 nm ≤ λ ≤ 400 nm. Within this range, peak effectiveness is observed at λ = 299 nm. More generally, promotion of NMSC appears to be dominated by radiation in the UV-B range (280 nm ≤ λ ≤ 320 nm).
NMSC effectiveness is quite small for wavelengths below about 280 nm, largely because radiation at these wavelengths does not penetrate deeply into human tissues. No data are available for wavelengths less than 250 nm, probably because at the time these values were identified there were few, if any opportunities for human exposure at these wavelengths. However, given the physics that govern the absorption of photons by human tissues, it is likely that radiation at wavelengths shorter than 250 nm represents a small risk of NMSC development.
Photochemical damage to human tissues is governed by the ability of photons to penetrate the tissue of interest and the ability of photons to damage tissue via photochemical reactions. These attributes both demonstrate strong wavelength dependence. In general, the ability to penetrate human tissues decreases with wavelength, while the opposite trend is evident in terms of the potential for photons to cause damage to human tissues. Given these opposing trends, it is common to observe a local maximum in effectiveness, as is evident in the NMSC effectiveness spectrum.
The relative contributions of ambient UV radiation to tissue damage will be governed by their relative spectral effectiveness and the availability of photons as a function of wavelength. As such, the product of relative spectral effectiveness and ambient solar spectrum provides an indication of the contributions of radiation at given wavelengths to promote a given biological response for a specific spectrum of incident radiation. This spectral behavior is defined as an “effectiveness spectrum.” Effectiveness spectra were defined by applying equation (3) to the data sets described above. In this equation, Eλ represents spectral irradiance and S(λ) represents relative spectral effectiveness.
This information, along with reference dose (DR) can be used to estimate a time of exposure to ambient solar radiation required to reach the TLVs (ACGIH, 2022). These exposure times were calculated using equation (4).
where t represents the time to reach the threshold limit value in seconds, DR is the reference dose (an equivalent dose of 30 J/m2 at 270 nm for eye and skin exposure and approximately 88 J/m2 for non-melanoma skin cancer [ACGIH, 2022]), and Δλ represents wavelength increment used in the calculation.
Results
Figures 4 and 5 illustrate the calculated effectiveness spectra for eye and skin exposure, respectively, based on Air Mass 1.0 and Air Mass 1.5. Figure 6 illustrates the corresponding calculated effectiveness spectrum for non-melanoma skin cancer.

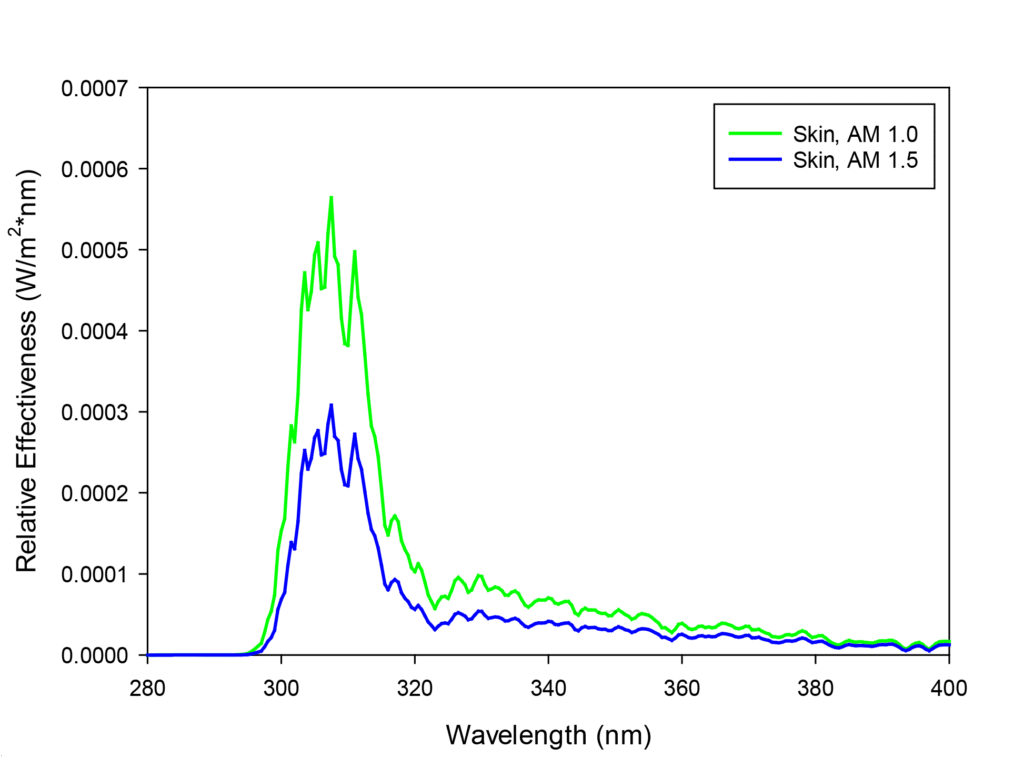
When examining these figures, maximum effectiveness for skin damage, eye damage and promotion of NMSC are observed at wavelengths of 307.5 nm, 306.5 nm and 311 nm, respectively. More generally, Figures 4-6 indicate that the majority of damage to these human tissues is associated with exposure to UV-B radiation. In addition, these figures show that contributions of radiation at wavelengths below approximately 290 nm are minor, largely because solar radiation at sea level does not include radiation in this wavelength range.
Using equation (2), the exposure time required to reach TLVs for the three biological responses can be calculated. The exposure times required to reach exposure limits for skin exposure, eye exposure and NMSC for Air Mass 1.0 are 24, 23 and 8 minutes respectively. The exposure times required to reach exposure limits for skin exposure, eye exposure and non-melanoma skin cancer for Air Mass 1.5 are 43, 42 and 14 minutes, respectively.
To put these values in context, it is important to recognize that the TLVs for skin and eye exposure are based on an assumed exposure time of eight hours per day. Properly designed GUV systems should yield human exposure below the TLVs for an eight-hour exposure period. Moreover, these calculations often are based on the assumption that a human will be exposed to the maximum (local) fluence rate in the room for the entire eight-hour exposure period. This implies that the exposed individual is stationary for the exposure period, and as such is probably a conservative representation of actual human exposure. Regardless, the calculations presented above allow these exposures to be related to human exposure to ambient solar UV radiation (i.e., “sunlight”), which is likely to be familiar to most people.
The Relationship to Ground Measurements of Solar Irradiance
To compare the spectral irradiance of Air Mass data to ambient data, spectral irradiance measurements were collected at three different locations using a portable spectroradiometer. These data were collected on cloudless days at approximately solar noon. The three locations were Las Canas, Dominican Republic (DR) on June 26; West Lafayette, IN on July 4, and Surfers Paradise, Australia on July 17.
Figure 1 illustrates spectral graphs produced from these data compared to the spectral graphs corresponding to Air Mass 1.0 and Air Mass 1.5. The data from these three locations are similar to the Air Mass 1.0 and Air Mass 1.5 spectra in shape and magnitude, and the Air Mass 1.0 and 1.5 spectra generally bracket the ambient solar spectra.
What Does this Mean for GUV Devices?
The calculations presented herein were conducted to facilitate quantitative comparisons between common forms of UV damage that are caused by exposure to ambient solar radiation with damage that corresponds to recommended exposure limits for UV-C radiation from GUV devices. A common barrier to implementation of GUV is the perception that installation of these systems will lead to increased risk of damage to human tissues, especially skin and eyes. The calculations presented above indicate that for properly designed GUV systems, the extent of damage to these external tissues, based on an assumed exposure period of eight hours, often based on the highest fluence rate in the exposure zone of the room, will be comparable to the damage done to these same tissues based on exposure to ambient sunlight for a period of 10’s of minutes. Moreover, GUV system designs can be developed to limit human exposure to well below the TLVs. Therefore, the risks to human tissues in association with GUV systems that are properly designed, installed and maintained is comparable, and probably smaller, than risks to UV exposure that are part of common human experiences.
Like any engineered system, GUV system designs should address the risks and benefits associated with the system. GUV systems have been proven to reduce human exposure to airborne and surface-associated pathogens; however, the general lack of understanding of these systems has been a barrier to their implementation. These fixtures present a risk of photochemical damage to external human tissues; however, proper design and implementation of these systems reduces that risk to a level that is consistent with or lower than common exposure scenarios, such as exposure to ambient sunlight.
References
- WHO (2025) COVID-19 Dashboard, https://data.who.int/dashboards/covid19/deaths.
- Center on Budget and Policy Priorities (2024), https://www.cbpp.org/research/economy/tracking-the-recovery-from-the-pandemic-recession, 3 April 2024.
- Hlávka J.; Rose, A. (2023) “COVID-19’s Total Cost to the U.S. Economy Will Reach $14 Trillion by End of 2023,” https://healthpolicy.usc.edu/article/covid-19s-total-cost-to-the-economy-in-us-will-reach-14-trillion-by-end-of-2023-new-research/.
- World Health Organization (2020) “Fighting COVID-19 could cost 500 times as much as pandemic prevention measures,” https://extranet.who.int/sph/fighting-covid-19-could-cost-500-times-much-pandemic-prevention-measures.
- Harvard University T.H. Chan School of Public Health (2024) “The Next Pandemic: Not if, but when,” https://hsph.harvard.edu/news/next-pandemic-not-if-but-when/, 12 September 2024.
- Faulkner, C.A.; Salsbury, T.I.; Abboushi, B.; Mouchref, C.; Singer, B.C.; Sohn, M.D.; Arnold, G. (2024) “Comparison of Effectiveness and Energy Use of Airborne Pathogen Mitigation Measures to Meet Clean Air Targets in a Prototypical Office Building,” Building and Environment, 257, 111466. doi.org/10.1016/j.buildenv.2024.111466.
- Nardell, E. (2021) “Air Disinfection for Airborne Infection Control with a Focus on COVID-19: Why Germicidal UV is Essential,” Photochemistry & Photobiology, 97, 3, 493-497. doi: 10.1111/php.13421.
- NREL (2025). Reference air mass 1.5 spectra. https://www.nrel.gov/grid/solar-resource/spectra-am1.5.html.
- ACGIH (2022) 2022 TLVs and BEIs. American Conference of Governmental Industrial Hygienists.
- International Commission on Non-Ionizing Radiation Protection, ICNIRP (2004) “ICNIRP Guidelines on limits of exposure to ultraviolet radiation of wavelengths between 180 nm and 400 nm (incoherent optical radiation), Health Physics, 87, 2, 171-186.
- International Organization for Standardization, ISO (2016) Photocarcinogenesis action spectrum (non-melanoma skin cancers); Geneva, Switzerland, 2016.

Ernest R. Blatchley III is the Lee A. Rieth Professor at Purdue University where he holds a joint faculty appointment in the Lyles School of Civil & Construction Engineering and the Division of Environmental & Ecological Engineering. The focus of research in the Blatchley group is on UV-based processes for treatment of water, air and surfaces. He serves as the president-elect of IUVA.