

By Cody Haag, Clean Sweep Group; George Holliday, MPH, and Kenneth Archulet, RN, CIC, Providence Holy Cross Medical Center; Weiming Tang, Ph.D., Institute for Global Health and Infectious Diseases, Gillings Global School of Public Health, University of North Carolina at Chapel Hill; and Pradyumna Swain, Ph.D., EIT2.0
Some of the newest iterations of UV-C room disinfection emitters boast autonomous or semi-autonomous capabilities, i.e. the ability to independently move around a target space. As a dedicated UV-C disinfection service provider, thus a user of UV-C emitters and a customer of emitter manufacturers, claims of faster disinfection times and near-elimination of shadows warranted investigation and scrutiny.
While there are some public data comparing select commercial UV-C emitters, the authors did not identify studies including autonomous emitters. More broadly, no literature was found comparing successive models of UV-C placement strategies, e.g. whole-room, spot, autonomous. To pursue due diligence, analyses were devised to isolate the impact of competing UV-C robot placement strategies, including autonomous placements.
Simulation analysis
The first analysis was a computer simulation constructed by calculating the UV-C intensity at each second with adjustments given the distance, angles and shadows from the emitter to sensor points with a cumulative tally for UV-C dose achieved. The simulation is accessible to readers at csgiusa.com/compareuv.
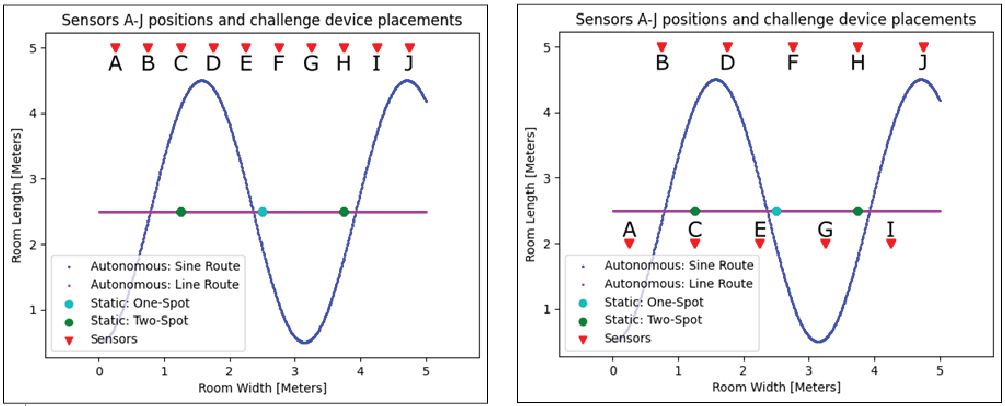
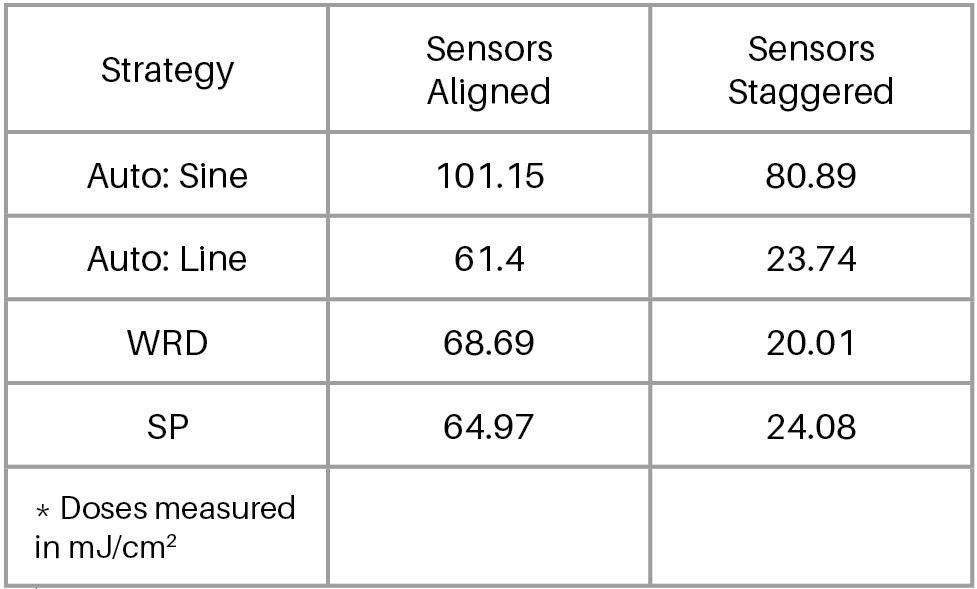
The tested simulation setting was a 5-meter by 5-meter space with 10 aligned or staggered sensor points. Four placement strategies are available in the simulation: Autonomous Sine, Autonomous Line, Static One-Spot and Static Two-Spot. All placement strategies assumed equal UV-C emitter intensity, 360-degree output and disinfection duration – placement strategy was the only differing factor. See Figure 1 for a simulation setting diagram with emitter and sensor positions.
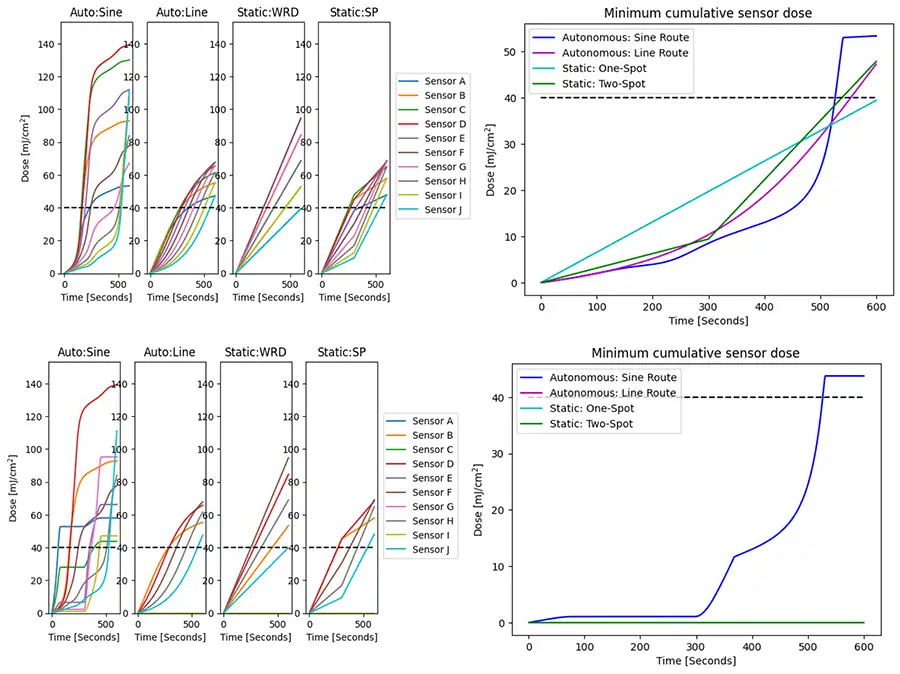
In both sensor configurations, the Autonomous Sine achieved the highest median dose (see Figure 2) and passed a dosage threshold on all sensors more quickly than the competing strategies (see Figure 3). In the tested simulation configurations, Autonomous Sine placement strategy best minimized the known physical limiters of UV-C with the lower distances and angles from the emitter to the sensors compared to the competing strategies.
Although the simulation is a simplified model of reality and does not fully represent the physical complexity of a hospital environment, nor include all UV-C irradiance factors, e.g. reflection, the placement strategies performed as expected given the known and measurable limits of UV-C irradiance and justified further investigation into the relative performance of the strategies.
Real-world settings
The second analysis was an empirical test in real-world hospital settings at Providence Holy Cross Medical Center in Mission Hills, California. The results were published in Infection Control and Hospital Epidemiology. 1 A commercially available UV-C emitter (Spectra 1000-RCT from TMG Health Technologies) was mounted to a remote-control platform; thus, a single device could replicate both autonomous and static placement strategies. Given the varying form factors and UV-C outputs among commercial emitters, the modified emitter (ME) was necessary to eliminate confounding related to emitter characteristics and isolate the effect of placement strategy. Additionally, a commercially available autonomous (CAE) emitter (OhmniClean 1080W from OhmniLabs) was tested for comparison to the modified emitter autonomous strategy to validate the ME as an adequate surrogate for this class of emitters.

Three placement strategies were compared: 1) an autonomous placement (ME-AUTO), defined as emitter traveling approximately 1 meter from all objects in room; 2) a static one-spot (ME-WRD), placed approximately center of the target space; and 3) a static two-spot (ME-SP), wherein the target space was broken into halves and therein placed approximately center for exactly half the disinfection duration (i.e., static two-spot was one emitter moved into two positions).
The competing placement strategies were tested in hospital spaces in which UV-C commonly is used: a patient room (C1), an operating room (C2) and an emergency room bay (C3). No conjoined spaces, e.g. a patient room with an ante room, were included as to not purposely advantage the autonomous strategy. In each of these settings, 10 electronic dosimeters (UV-CKEY from EIT) were placed in an approximate grid-like configuration throughout the target space, including on a variety of surfaces, including inner bed rails (see Figure 4) and computer workstations.
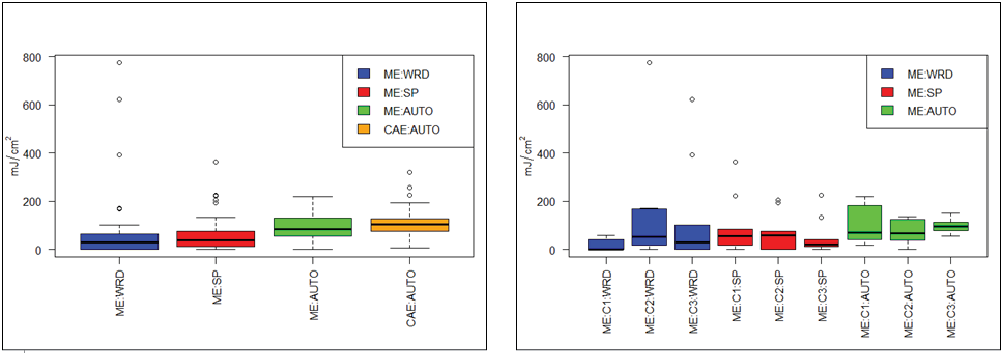
In aggregate and in each challenge setting, the ME-AUTO strategy achieved a significantly higher median UV-C dose compared to the ME-WRD and ME-SP strategies (see Figure 5). Similar to the simulated results, the distance and shadowing was lowest with the ME-AUTO strategy. Last, there was no significant difference in aggregate median dose between ME-AUTO and CAE-AUTO, which provided evidence for the ME-AUTO being a sufficient experimental analog for a commercial autonomous emitter.
Limitations and findings
There were substantial limitations of the real-world experiment. First, 10 sensors per challenge space is an incomplete measure of the dose achieved on hospital surfaces. Second, limitations from the sensor themselves in measuring at highly-angled or low-intensity exposures may have slightly undercounted UV-C dose at some emitter positions.
The findings of the computer simulation and real-world comparisons of emitter placements demonstrated the following:
- Autonomous placement strategies generally lead to higher overall UV-C doses.
- Static placement strategies simultaneously over- and under-dose surfaces.
- The autonomous strategies achieved higher UV-C doses on surfaces that were distant, angled or shadowed to the static placements.
Though it was outside the scope of this research, it is likely the elevated UV-C dose from the autonomous UV-C strategies will translate into cleaner hospital rooms; however, it is less clear if incrementally cleaner rooms will reduce hospital-acquired infections beyond those achieved with static UV-C emitters. But, autonomous strategies will exceed a minimum dose threshold on all surfaces in a disinfected space given the variance of dose from static placements; thus, autonomous placements may complete a disinfection cycle sooner than static placements. More importantly, a carefully constructed autonomous pathway is not inhibited by shadows, leading to a more consistent application of UV-C throughout a target space. This research concludes organizations can expect to disinfect rooms faster and more thoroughly with autonomous UV-C emitters than with static UV-C emitters.
References
- Haag CW, Holliday G, Archulet K, Tang W. Comparing UV-C dosages of emitter placement strategies in a community hospital setting. Infection Control & Hospital Epidemiology. 2023;44(9):1505-1507. doi:10.1017/ice.2022.282
Author’s note: An earlier version of this study was published online in Infection Control and Hospital Epidemiology, titled “Comparing UV-C dosages of emitter placement strategies in a community hospital setting” on December 16, 2022, available at: https://www.cambridge.org/core/journals/infection-control-and-hospital-epidemiology/article/abs/comparing-uvc-dosages-of-emitter-placement-strategies-in-a-community-hospital-setting/33E358712EE7280E492ECE43829114E9.

Cody Haag is the vice president of Research and Development at Clean Sweep Group, Inc. (CSGI), a UV robots-as-a-service (RaaS) provider. Haag developed CSGI’s Triage implementation strategy and software, which for over a decade has contributed to their success in reducing hospital-acquired infections (HAIs) for customers. He has authored articles on UV disinfection in ICHE, AJIC and other respected publications.